
Over the past several years I have actively cultivated my appreciation of what interferes with optimal team performance, and spent a considerable amount of time investigating possible solutions. I had the privilege recently to lead a workshop on team development with the Wake Forest Orthopaedic residents, and it became very clear to me that encountering conflict on teams during the course of our daily work is not limited to a generation of those, like myself, who trained under a more traditional leadership paradigm, when one’s team actually meant a “group of individuals whose job it was to support the surgeon!” Although millennials may at first glance be easier going and adaptable, make no mistake about it, they too are frustrated by what they almost universally view as insurmountable impediments to building a high performing team. One participant in his chief year expressed a feeling of complete impotence when it came to how to make things better—settling on complete resignation, “I decided it is a futile effort, and so I just accept dysfunction.”
During the course of my visit I truly appreciated the impact of exigent cultural and systemic barriers to a synergistic team and esprit de corps, including lack of engagement by union and/or temporary staff, lack of standing as “residents” compared to their attendings (and a perceived lack of respect), not working with the same people from day to day or week to week, and numerous process/operational inefficiencies inherent in a large university hospital.
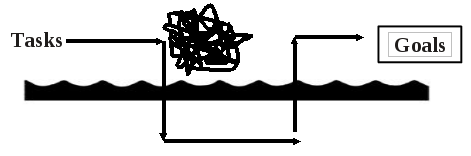
So how on earth can we “move the needle” amidst such structural and process-related problems? Well, the “Waterline Model” provides some insight as to how to deal with team challenges and breakdowns. The model identifies four aspects of team and organizational life that operate under the waterline and that might create a roadblock to optimal performance: 1) Structure; 2) Process; 3) Interpersonal Issues; and 4) Intrapersonal Issues. The Waterline Model invites you to switch from a focus on task to a focus on process, and to dive beneath the water to better understand what’s happening and how to address it. This can obviate often frustrating team dynamics when a problem occurs or is recurring.
(https://stillpointleadership.com/waterline-model/)

The Waterline Model can help you distinguish between the common issues that bog teams down, and be deliberate about how you address them. Firstly, whatever breakdown your team is facing, it almost always has to do with something in the first two categories—a structural or process issue. There may be system issues like restricted duties (as might be dictated for union workers) and ineffective leadership (a poor OR supervisor for example), or process issues like ineffective communication, poor alignment and clarity regarding roles and responsibilities, and lack of a feedback loop, which prohibits process improvement. How often do you find yourself bemoaning that you always use the same instrument or suture, and yet it never gets corrected on your “preference card”?
Individual resolve too often will not remediate these issues, but despite frustration, and perhaps feelings of disempowerment due to an inability to instantaneously fix after diagnosing the problem, the conflict or problem is rarely personal. In fact, these problems just below the waterline represent issues that may only get solved if the team finds a way to collectively push for a solution. Such a unified voice, in fact, can build team identity and a sense of empowerment, and it’s often far more compelling as compared to our solitary complaint! Further, in the process of developing a shared appreciation of what structural and process constraints exist, and collectively owning an aspirational commitment to resolution, whatever interpersonal conflict may exist on a team, may resolve as well. So as the physician-surgeon, we should aspire to sharing in the process of identifying structural or process problems—with our team—and working towards being part of the solution. The emphasis here is building a team’s voice with gravitas, and rejecting the temptation to simply express frustration or complain.
Of course, problems on teams are rarely limited to the first two categories. In fact, more often than not, a dysfunctional team struggles with interpersonal conflict, such as a personality clash or misunderstanding, or an intrapersonal challenge such as poor self-awareness or self-management. We and our colleagues bring problems to work, and the stress of everyday life may interfere with being the best version of ourselves at all times. One of the residents at Wake shared a story of a radiology technologist who sat on her chair reading a book in between C-arm imaging during a hip ORIF. He was frustrated by her seeming disinterest and failure to engage. Of course, that was his narrative. When I asked him whether he thought there was any way he could move the needle in that context, he replied “not a chance—that problem was not solvable at my pay grade.”
I thought about that on my flight home, particularly in the context of my own previous experience a few years ago on a really dysfunctional team. At the end of 4 total shoulder replacements, during which the scrub technician passed instruments across the OR table, I asked that she move her table to my side of the table for the next case, an ORIF of a greater tuberosity fracture. I thought it made sense and would be more helpful to me to have her next to me. She did not see it that way and responded, “No. In fact, I don’t even want to be in here for that case.”
How would you have responded?
I worked with this tech once every 2 weeks at the time. Although quite competent, she was typically irreverent and unfriendly. It took all my energy to remain silent most days. On this occasion, I could just ignore her and hope she moved the table. I could capitulate and avoid the conflict. I could be provoked by her recant and say “Fine; please find someone who does.” The latter option— my response—reflected, in hindsight, a feeling of not only impotence, shared by the chief resident—thinking “I can’t even begin to move this needle”—but also an emotional reaction to what I perceived was insubordinate behavior.
I appreciate now that I had missed an opportunity to move the needle then, just as many of us may miss similar opportunities simply because of too narrow a prism. Indeed, if we feel frustration with a co-worker and begin to craft a narrative in our mind, which is predicated on blame—too lazy, too indifferent, not committed, or whatever—we miss the opportunity to greet the “conflict” with curiosity and engage. Leveraging conflict is the most effective way to build mutual understanding and respect. Engagement is the starting point for moving the needle because in so doing we demonstrate an interest in the other party. This begins the process of building trust and our subsequent encouragement of candor. Rather than thinking “what’s the matter with him/her” ask “what matters to him/her?” While it is understandable to feel impotent with an unengaged seemingly disinterested party, one cannot predict that attempting to build relationship equity will be fruitless.
Based on my experience, I have come to believe that we as the surgeons are capable of moving the needle, one person at a time, if we are willing to change our optics and look through our prism with empathy and curiosity. Our actions create our reality. Deliberately inviting a team member to embrace being part of the team, and then affirming their value and encouraging their feedback is a skill that we can develop. Dive beneath the waterline at the deepest levels, and you will find that it is where high performing teams practice to achieve their goals.

{kind=link}
Dear Dr. Tamaino,
I read your paper as one who is now semi=retired following 40 years as a practicing ortho hand surgeon. Having practiced and trained in 4 states. 4 trauma hospitals, 5 VA’s, plus my private practice. I have seen multiple environments==joyous, union bureaucracy, warm & friendly. OR’s with surgeons who are a true pleasure to be around; surgeons who are bullies, arrogant, and just plain jerks. I think the answer to creating a team approach often lies in letting the other members of the team some input in the way things run, but the firm understanding that the most important person in that OR is the person lying on the table.Those who can’t grasp that unfortunately probably have to leave including us.
My best wishes for a timely paper.
Douglas A. Drake, MD